Data breach reporting is the legal process of notifying regulators, affected individuals, and, in some cases, the public when unauthorized access to protected data occurs. Under every major privacy regulation in force today, organizations that experience a qualifying breach face mandatory disclosure deadlines, designated reporting authorities, and escalating penalties for non-compliance.
The challenge is that no single rulebook governs data breach reporting globally. A healthcare provider in the United States answers to HIPAA and HHS OCR. A SaaS company handling EU customer data answers to GDPR and the relevant Data Protection Authority. A publicly traded company answers to the SEC. A business that collects California consumer data is subject to the CCPA. In many cases, a single breach triggers simultaneous obligations under multiple frameworks, each with its own timeline, form, and threshold for what counts as reportable.
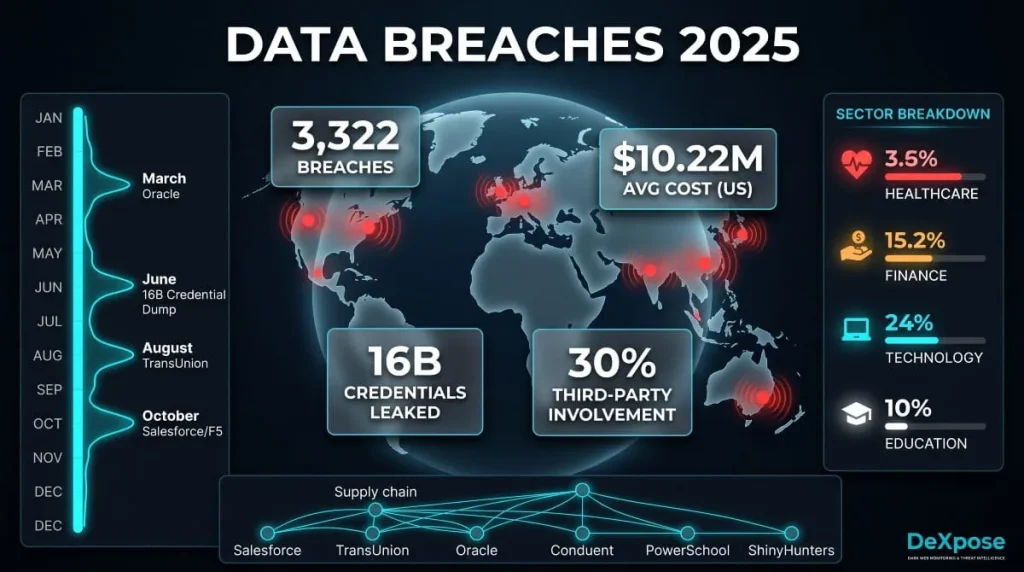
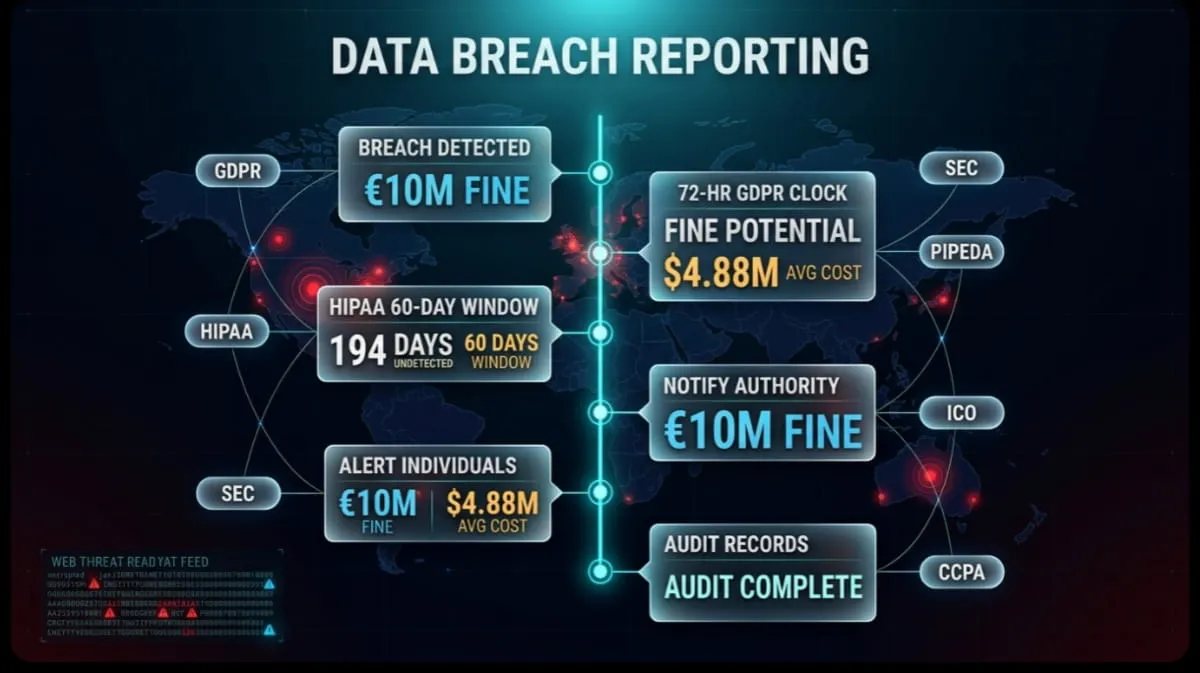
What unifies all of them is urgency. The IBM Cost of a Data Breach Report 2024 found that the average cost of a data breach reached $4.88 million, the highest figure ever recorded, with delayed reporting and slow containment directly amplifying that cost. Organizations that contained a breach in under 200 days saved an average of $1.1 million compared to those that took longer. Regulators have taken note: the global trend across every jurisdiction is shorter deadlines, stricter enforcement, and higher fines for organizations that treat notification as an afterthought.
This guide covers everything compliance officers, security teams, and business owners need to know: which regulations apply, how long you have to report under each one, who you report to, what forms are required, and what happens if you miss the deadline.
What Is Data Breach Reporting?
Data breach reporting is the formal process by which an organization discloses a security incident involving unauthorized access, acquisition, or exposure of protected personal data to relevant regulatory authorities, affected individuals, and, in some cases, the broader public. It is a compliance obligation, not a discretionary action, triggered the moment an organization determines that a qualifying incident has occurred.
The specific mechanics of reporting vary by jurisdiction and regulation, but the core obligation is consistent: once a breach crosses a defined threshold of harm or sensitivity, the clock starts. Organizations must assess the incident, determine whether it meets the legal definition of a reportable event, identify the correct authorities, and file notification within a mandated timeframe. Failure at any of these steps carries legal and financial consequences.
Definition of a Reportable Data Breach
A reportable data breach is a security incident in which personal, protected, or sensitive data has been accessed, disclosed, altered, or destroyed without authorization, and where that exposure creates a real or likely risk of harm to the individuals whose data was affected.
The key Word in that definition is risk. Not every unauthorized access event qualifies as reportable. What separates a reportable breach from a contained security incident is whether the compromised data was actually accessible to, or acquired by, an unauthorized party, and whether that exposure poses a meaningful risk of harm. Regulators across GDPR, HIPAA, PIPEDA, and other frameworks have set their reporting thresholds based on this harm-risk principle rather than on the breach event itself.
Under GDPR, for instance, a reportable personal data breach is defined as a breach of security leading to accidental or unlawful destruction, loss, alteration, unauthorized disclosure of, or access to, personal data. HIPAA defines a reportable breach as impermissible use or disclosure of protected health information that compromises its security or privacy, with a built-in presumption that any impermissible disclosure is a breach unless the covered entity can demonstrate through a documented four-factor risk assessment that the probability of data compromise is low.
What Qualifies as a Notifiable Breach vs. a Non-Reportable Incident
The line between a notifiable breach and a contained security incident comes down to two factors: the nature of the data involved and the realistic probability that it was accessed or used by an unauthorized party.
A notifiable breach typically involves data categories that regulators treat as high-risk by default: full names combined with Social Security numbers, financial account credentials, protected health information, biometric data, login credentials, or government-issued identification numbers. When data of this type is involved in an unauthorized disclosure, the presumption in most jurisdictions is that notification is required unless the organization can affirmatively demonstrate otherwise.
A non-reportable incident, by contrast, is usually a situation in which unauthorized access occurred. Still, the data was rendered unreadable through strong encryption, for example, or where the data involved carries no realistic harm potential on its own, such as publicly available information or anonymized records. Under HIPAA’s Safe Harbor provision, a breach involving encrypted PHI where the decryption key was not also compromised is explicitly excluded from breach notification requirements. GDPR similarly allows organizations to determine that notification to affected individuals is unnecessary if the breach is unlikely to result in a high risk to their rights and freedoms. However, regulator notification may still be required even in that scenario.
The practical implication is that every security incident requires a documented risk assessment before an organization can conclude it is non-reportable. Assuming an incident doesn’t need to be reported without formal analysis is, in itself, a compliance failure.
Do All Data Breaches Need to Be Reported?
No, but the threshold for exemption is narrow, and the burden of proof sits entirely with the organization. Every major privacy regulation establishes a harm-risk standard that determines whether a breach triggers notification. Still, none of them allow organizations to simply decide a breach is minor without documentation to support that conclusion.
Under HIPAA, the presumption is that every impermissible disclosure of PHI is reportable unless the covered entity or business associate can demonstrate low probability of compromise across four specific factors: the nature and extent of the PHI involved, who accessed it, whether it was actually acquired or viewed, and the extent to which risk has been mitigated. This presumption-of-breach rule was introduced precisely to prevent organizations from reflexively classifying incidents as non-reportable to avoid disclosure obligations.
GDPR takes a two-tier approach. Breaches must be reported to the supervisory authority unless they are unlikely to result in a risk to the rights and freedoms of natural persons. Breaches that are likely to result in a high risk require notification to affected individuals as well. This means an organization can sometimes avoid notifying data subjects while still being required to report to its Data Protection Authority; the two obligations operate independently.
The practical answer for any security team is to treat every incident involving personal data as presumptively reportable until a documented assessment concludes otherwise, and to retain that documentation, because regulators will ask for it.
Who Determines If a Breach Is Reportable?
The organization that controls the data, the data controller under GDPR, the covered entity or business associate under HIPAA, or the business under CCPA, is responsible for making the initial determination of whether a breach is reportable. That determination must be made by qualified personnel, documented formally, and completed within the timeframe required by the applicable regulation, because the reporting clock often begins when the organization becomes aware of the incident, not when the investigation concludes.
In practice, this means the decision sits with the organization’s privacy officer, legal counsel, CISO, or a designated incident response team. Many organizations use a structured risk assessment framework, either built internally or prescribed by regulation, to evaluate each incident against the criteria for reportability. HIPAA’s four-factor risk assessment is the most codified example of this, but the European Data Protection Board’s guidance documents provide similarly detailed frameworks for DPA notification decisions.
Critically, being unsure whether a breach is reportable is not a valid reason to delay assessment. Regulators in both the US and the EU have issued enforcement actions against organizations that knew of a breach but delayed the determination of reportability while conducting broader investigations. The assessment and the investigation can, and should, run in parallel.
Data Breach Reporting Timelines by Regulation
The single most consequential variable in data breach reporting is time. Every major privacy and security regulation sets a mandatory notification deadline. In most cases, that clock starts running the moment an organization becomes aware of the incident, not when the investigation is complete. Missing a deadline is itself a compliance violation, independent of the breach that triggered it.

The timelines below reflect the current requirements under each framework. Organizations subject to multiple regulations, such as a US healthcare company with EU customers, must satisfy all applicable deadlines simultaneously, defaulting to whichever is most restrictive.
GDPR, 72-Hour Rule Explained
Under the General Data Protection Regulation, a personal data breach must be reported to the competent supervisory authority within 72 hours of the data controller becoming aware of it. This is one of the strictest breach notification deadlines in the world, and it applies regardless of whether the investigation is complete at the time of filing.
The 72-hour window is not a deadline for completing the notification; it is a deadline for beginning it. GDPR explicitly permits organizations to submit an initial notification with the information available at the time and supplement it with additional details as the investigation progresses. What regulators penalize is silence: failing to notify at all, or notifying significantly late without documented justification for the delay.
If notification cannot be made within 72 hours, the organization must file the report anyway and include a reasoned explanation for the delay. Supervisory authorities across the EU have consistently held that an ongoing internal investigation is not, in itself, sufficient justification for missing the deadline. The clock is designed to be uncomfortable, because the individuals whose data was compromised need to be protected quickly.
When a breach is also likely to pose a high risk to data subjects’ rights and freedoms, the GDPR imposes a second obligation: notification to the affected individuals themselves, which must occur without undue delay. There is no fixed number of hours prescribed for this second tier, but regulators expect it to closely follow the supervisory authority notification.
HIPAA, When Must a Breach Be Reported?
HIPAA breach reporting operates on two separate timelines depending on the scale of the breach, and both are measured from the date of discovery rather than the date of occurrence.
For breaches affecting 500 or more individuals, covered entities must notify HHS OCR and affected individuals within 60 days of discovering the breach. This 60-day window is a hard cap, not a target. Notification to the affected individuals must happen simultaneously. If the breach affects residents of a state or jurisdiction served by prominent media outlets, a press notice must also be issued within the same 60-day period.
For breaches affecting fewer than 500 individuals, covered entities have until 60 days after the end of the calendar year in which the breach was discovered to notify HHS OCR. Individual notification still occurs within 60 days of discovery. This annual reporting pathway is sometimes misread as flexibility; it is not. Individual notification is still due within 60 days of discovery, regardless of the breach’s size. Only the HHS OCR submission is deferred to the annual log.
Business associates under HIPAA must notify the covered entity of a breach within 60 days of discovery, though contracts between the parties often require faster notification; 10 or 30 days is common. HIPAA itself sets 60 days as the ceiling, not the floor.
CCPA, California Breach Reporting Deadlines
The California Consumer Privacy Act, as amended by the California Privacy Rights Act (CPRA), does not specify a fixed number of hours or days for breach notification, unlike the GDPR. Instead, it requires that notification to affected California residents be made as soon as possible, without unreasonable delay, following discovery of a qualifying breach.
In practice, California’s Attorney General and courts have interpreted this standard to mean that notification should occur within 30 to 45 days in most circumstances. Delays beyond that range require a documented justification, typically an active law enforcement investigation that would be compromised by early disclosure, or a legitimate need to determine the scope of the breach before notification can be accurate.
CCPA breach liability is triggered specifically when a business fails to implement and maintain reasonable security measures and a breach of unencrypted personal information results. This means the regulation’s teeth are primarily in civil litigation and regulatory enforcement of security standards, with breach notification serving as the disclosure mechanism that enables enforcement.
PIPEDA, Real Risk of Significant Harm Standard
Canada’s Personal Information Protection and Electronic Documents Act requires mandatory breach reporting when a breach creates a real risk of significant harm to affected individuals. This harm-risk threshold is the central determination; unlike GDPR’s broad notification requirement, PIPEDA does not require reporting for every breach involving personal data, only those that clear the significant harm bar.
Significant harm under PIPEDA includes bodily harm, humiliation, damage to reputation or relationships, financial loss, identity theft, negative effects on a credit record, and damage to or loss of employment, business, or professional opportunities. Organizations must assess each breach against these criteria and document their reasoning, because the Office of the Privacy Commissioner of Canada (OPC) may request that documentation during an investigation.
When the significant harm threshold is met, PIPEDA requires notification to the OPC and affected individuals as soon as feasible after determining that a real risk of significant harm exists. The OPC’s guidance makes clear that “as soon as feasible” means promptly and that extended delays for the sake of investigative completeness are not acceptable. Organizations must also maintain a record of every breach, regardless of whether it meets the reporting threshold, for at least 24 months.
SEC, Cyber Breach Reporting Requirements for Public Companies
The Securities and Exchange Commission’s cybersecurity disclosure rules, which took effect in December 2023, require publicly traded companies to report material cybersecurity incidents within four business days of determining that the incident is material. This is one of the most significant expansions of breach reporting obligations for the corporate sector in recent US regulatory history.
Materiality under the SEC framework follows the standard used across securities law: an incident is material if a reasonable investor would consider it important in making an investment decision. Companies are responsible for making that determination promptly; the four-day clock starts from the date of the materiality determination, not from the date of discovery. This creates a practical incentive to complete materiality assessments quickly, since delay in the assessment does not pause the reporting clock once a conclusion is reached.
The disclosure is made via Form 8-K, Item 1.05. It must describe the material aspects of the incident’s nature, scope, and timing, as well as its material impact or reasonably likely material impact on the company. The SEC has made clear it will scrutinize both the timeliness of disclosure and whether companies are accurately characterizing incidents as immaterial to avoid the reporting obligation.
FCC Data Breach Reporting Rules
The Federal Communications Commission’s updated data breach reporting rules, which came into force in 2024, apply to telecommunications carriers and require notification on three parallel tracks: to the FBI and Secret Service, to the FCC itself, and to affected customers.
Law enforcement notification must occur within seven business days of a carrier reasonably determining that a breach has occurred. Customer notification follows after the law enforcement notification period, unless law enforcement requests a delay, which can be granted for up to 30 days and extended in extraordinary circumstances. The FCC itself must be notified simultaneously with customers.
The rules apply to breaches of Customer Proprietary Network Information (CPNI), the data carriers collect about customers’ use of telecommunications services, and represent a significant tightening of requirements that had remained largely unchanged since 2007. The updated framework removes a provision that previously allowed carriers to delay customer notification whenever law enforcement was involved, replacing it with a structured timeline that preserves law enforcement coordination while ensuring customers are notified within a defined window.
DOD / US-CERT, PII Breach Reporting Timeframes
Within the US federal government, the Department of Defense and other agencies are bound by OMB Memorandum M-17-12, which requires that all breaches involving Personally Identifiable Information be reported to US-CERT within one hour of discovery. This is the most aggressive breach reporting deadline in any regulatory framework currently in force, and it is not aspirational. Federal agencies are expected to have incident response capabilities in place that enable one-hour notification.
Following the initial US-CERT notification, DOD organizations conduct a more detailed breach analysis to determine whether the PII involved creates a risk of harm to affected individuals. If it does, affected individuals must be notified within 10 days of the breach determination. The agency’s Senior Agency Official for Privacy, or a designated privacy officer, is responsible for overseeing the harm analysis and notification process.
The one-hour rule reflects the federal government’s posture that early warning to central cybersecurity authorities is a prerequisite to effective incident response at scale, not a formality to be completed after the internal investigation concludes.
Australia, OAIC Notifiable Data Breaches Timeline
Australia’s Notifiable Data Breaches (NDB) scheme, administered by the Office of the Australian Information Commissioner (OAIC), requires organizations covered by the Privacy Act 1988 to notify the OAIC and affected individuals as soon as practicable, and no later than 30 days after becoming aware that there are reasonable grounds to believe an eligible data breach has occurred.
An eligible data breach under the NDB scheme is likely to result in serious harm to any individual whose information was involved. If an organization suspects a breach has occurred but is not yet certain, it has 30 days to conduct an assessment of whether the incident constitutes an eligible data breach. That 30-day assessment window is itself a deadline; organizations cannot conduct an indefinite investigation to avoid triggering notification obligations.
The OAIC’s enforcement posture has sharpened considerably in recent years. Following high-profile breaches affecting Australian consumers at Optus and Medibank in 2022, the Australian government increased the maximum penalties for serious or repeated privacy breaches to AU$50 million, three times the value of any benefit obtained from the misuse of information, or 30 percent of an entity’s adjusted turnover, whichever is greatest.
UK GDPR / ICO, 72-Hour Reporting to the ICO
Following Brexit, the United Kingdom enacted its own version of GDPR, the UK GDPR, which mirrors the EU regulation’s 72-hour notification requirement almost exactly. Organizations operating in the UK must report a personal data breach to the Information Commissioner’s Office within 72 hours of becoming aware of it, provided the breach is likely to result in a risk to the rights and freedoms of individuals.
As with EU GDPR, the 72-hour clock begins at the point of awareness, and organizations are permitted to submit an initial report with partial information and supplement it as the investigation develops. The ICO has published detailed guidance on what the initial report must contain, the nature of the breach, the approximate number of individuals affected, the likely consequences, and the measures taken or proposed to address it, and expects organizations to have this information largely ready through pre-existing incident response documentation.
The ICO’s enforcement record is significant. It has issued fines ranging from hundreds of thousands to millions of pounds for late, inadequate, or no notification. It has also made clear that proactive engagement- contacting the ICO early, even before the 72-hour deadline, when a major breach is suspected- is viewed more favorably than waiting until the last moment with a complete report.
Who Do You Report a Data Breach To?
Who you report a data breach to depends on the type of data compromised, the industry you operate in, and the jurisdictions where your affected individuals reside. There is no single universal authority; most organizations subject to a significant breach will need to notify multiple bodies simultaneously, each with its own submission process, required format, and deadline.

The question of where to report is inseparable from the question of which regulation governs the data involved. A breach affecting employee health records triggers HIPAA and HHS OCR. The same breach at a publicly traded company may also trigger SEC disclosure obligations. If those employees are California residents, CCPA notification requirements apply on top. Mapping your reporting obligations before a breach occurs, not during one, is the difference between an orderly response and a compliance crisis.
Reporting to the ICO (UK)
In the United Kingdom, personal data breaches likely to pose a risk to individuals’ rights and freedoms must be reported to the Information Commissioner’s Office. The ICO is the UK’s independent data protection regulator and the sole supervisory authority for UK GDPR breach notifications; organizations do not report to multiple UK bodies for the same breach.
Notification is submitted through the ICO’s online breach reporting portal at ico.org.uk. The report must include the nature of the breach, the categories and approximate number of individuals and personal data records affected, the likely consequences of the breach, and the measures taken or proposed to address it. Organizations are not required to have complete answers to all of these questions before filing; the ICO expects initial reports within 72 hours and accepts supplementary information as the investigation progresses.
The ICO distinguishes between breaches that require only regulator notification and those that also require notification to affected individuals. If a breach is likely to pose a high risk to individuals, including identity theft, financial loss, discrimination, or reputational damage, both the ICO and the affected individuals must be notified. If the risk is present but not high, only the ICO notification is required. If the breach is unlikely to result in any risk, no notification is legally required, though the breach must still be documented internally.
Reporting to HHS OCR (HIPAA Breaches)
Under HIPAA, covered entities, healthcare providers, health plans, and healthcare clearinghouses report breaches of protected health information to the US Department of Health and Human Services Office for Civil Rights. HHS OCR is the enforcement authority for HIPAA’s Breach Notification Rule, and all formal breach submissions are made through its dedicated online portal at ocrportal.hhs.gov.
For breaches affecting 500 or more individuals, the covered entity submits the breach report to HHS OCR within 60 days of discovery, simultaneously with notifying affected individuals. For breaches affecting fewer than 500 individuals, covered entities log the breach and submit an annual report to HHS OCR within 60 days after the end of the calendar year in which the breach was discovered.
HHS OCR publishes all reported breaches affecting 500 or more individuals on its public breach portal, commonly referred to in the industry as the HIPAA Wall of Shame. This public disclosure is itself a compliance mechanism: it creates reputational accountability and allows the public to see which covered entities have experienced significant incidents. As of 2024, HHS OCR had investigated over 38,000 HIPAA complaints and resolved cases resulting in more than $145 million in penalties, making it one of the most active data breach enforcement bodies in the United States.
Reporting to the SEC
Publicly traded companies in the United States report material cybersecurity incidents to the Securities and Exchange Commission via Form 8-K, Item 1.05. The SEC’s cybersecurity disclosure rules, effective December 2023, require this filing within four business days of the company determining that a cybersecurity incident is material, meaning a reasonable investor would consider it significant when making an investment decision.
The Form 8-K disclosure must describe the material aspects of the incident: its nature, scope, and timing, the data or systems affected, and the actual or reasonably likely material impact on the company’s financial condition or operations. Companies are not required to disclose specific technical details that would compromise ongoing remediation or assist threat actors. Still, they cannot use that carve-out as a general exemption from substantive disclosure.
In addition to Form 8-K incident reporting, the SEC requires annual disclosure of a company’s cybersecurity risk management program, governance structure, and board-level oversight of cyber risk via Form 10-K. The two reporting streams, incident disclosure and program disclosure, are designed to give investors a complete picture of how a company manages cyber risk over time, not just when a breach occurs.
Reporting PHI Breaches: Covered Entity Obligations
When protected health information is breached, covered entities under HIPAA carry a layered set of reporting obligations that extend beyond HHS OCR. The Breach Notification Rule requires notification to three distinct parties: affected individuals, HHS OCR, and in cases involving large breaches, prominent media outlets serving the affected area.
Notification to affected individuals must be provided in written form, typically by first-class mail to the individual’s last known address, within 60 days of discovery. If the covered entity has insufficient contact information for 10 or more individuals, substitute notice is required, either by posting on the entity’s website for 90 days or by major print or broadcast media. If the breach affects 500 or more residents of a specific state or jurisdiction, a media notice must also be issued to prominent media outlets in that area within the same 60-day window.
Business associates that discover a breach involving PHI are required to notify the covered entity, not HHS OCR directly. The covered entity retains primary responsibility for notifying the regulator and individuals, but the business associate must provide the covered entity with the information needed to meet those obligations. This division of responsibility is typically formalized in the Business Associate Agreement between the parties, and gaps in that agreement are a common point of enforcement scrutiny following a breach.
Reporting PII Breaches to US-CERT and DOD Authorities
Federal agencies and Department of Defense organizations that experience a breach involving Personally Identifiable Information report to the Cybersecurity and Infrastructure Security Agency’s United States Computer Emergency Readiness Team, US-CERT, within one hour of discovery. This one-hour requirement, established under OMB Memorandum M-17-12, applies to all federal civilian executive branch agencies and is among the most demanding breach notification timelines in any regulatory framework.
The initial US-CERT notification is a security alert, not a comprehensive breach report; it is designed to trigger coordinated federal incident response as quickly as possible. A more detailed incident report follows as the agency’s investigation develops. DOD-specific guidance further requires that the agency’s Senior Agency Official for Privacy assess the breach’s potential for harm and, where a risk of harm to affected individuals is identified, initiate individual notification within 10 days.
The rationale for the one-hour standard is systemic: federal agencies handle PII at scale, and a breach at one agency can have cascading implications for connected systems across the government. Early warning to US-CERT is treated as a prerequisite to coordinated national-level response, not merely an administrative formality.
Reporting a Data Breach to the Social Security Administration
When a data breach exposes Social Security numbers, whether as a standalone element or as part of a broader record, the Social Security Administration is not a primary breach reporting authority, unlike HHS OCR or the ICO. There is no federal regulatory requirement to file a breach report directly with the SSA solely because SSNs were compromised.
The SSA’s role in breach response is primarily consumer-facing: it provides resources and guidance for individuals whose Social Security numbers have been exposed, including the ability to place a credit freeze, enroll in identity monitoring programs, and, in cases of documented identity theft, obtain a new Social Security number. Affected individuals can report SSN misuse to the SSA’s Office of Inspector General and to the Federal Trade Commission via IdentityTheft.gov.
Organizations that experience a breach involving SSNs must still meet their state-level breach notification obligations; every US state has a breach notification law that specifically includes SSNs as a trigger data element and requires notification to affected individuals so they can take protective action. The notification itself, rather than a regulator filing with the SSA, is the primary compliance obligation when SSNs are the data at risk.
State-Level Reporting Authorities in the US
All 50 US states, the District of Columbia, Puerto Rico, and the US Virgin Islands have enacted data breach notification laws, each with its own definition of covered data, trigger threshold, notification deadline, and designated authority. This patchwork of state laws means that a single breach affecting residents across multiple states can simultaneously trigger dozens of distinct notification obligations.
In most states, the primary reporting authority is the state Attorney General. Some states, including California, New York, and Texas, also require notification to the AG’s office in addition to individual notification. In contrast, others require only individual notification with no direct regulator filing. New York’s SHIELD Act, for example, requires notification to the AG, the Department of State, and the Division of State Police for breaches affecting New York residents, in addition to the affected individuals themselves.
The most important variable across state laws is the definition of personal information that triggers notification. Most states include the combination of name plus SSN, financial account numbers, or driver’s license numbers as the baseline trigger. An increasing number of states, including California, Virginia, and Colorado, have expanded the definition to include health data, biometric identifiers, precise geolocation, login credentials, and genetic data. Organizations operating nationally must map their breach response to the most expansive definition applicable to any state where affected individuals reside.
Where to Report a Data Breach in Australia
In Australia, organizations covered by the Privacy Act 1988 report eligible data breaches to the Office of the Australian Information Commissioner. The OAIC administers the Notifiable Data Breaches scheme and is the sole federal regulator for privacy breach notifications. Reports are submitted through the OAIC’s online notification form, and the organization must simultaneously notify affected individuals as soon as practicable.
The OAIC notification must include the organisation’s identity and contact details, a description of the breach, the types of information involved, and the steps the organisation recommends that affected individuals take in response. If it is not practicable to notify each affected individual directly, for example due to insufficient contact information, the organisation must publish a notice on its website that remains accessible for at least 90 days.
Australia’s sector-specific regulators also play a role in breach response. The Australian Prudential Regulation Authority (APRA) governs breach obligations for banks, insurers, and superannuation funds under its CPS 234 information security standard. The Australian Securities and Investments Commission (ASIC) administers breach reporting requirements for financial services licensees under RG 78. Organizations in regulated sectors must satisfy both the OAIC’s requirements and their sector regulator’s obligations, which may differ in terms of thresholds, timelines, and submission formats.
Reporting to FERPA, FDA, and Other Sector-Specific Regulators
Beyond the major horizontal privacy frameworks, a range of US sector-specific regulations impose breach reporting obligations on organizations in education, healthcare device manufacturing, financial services, and critical infrastructure, each with a distinct reporting authority and procedural requirements.
Under the Family Educational Rights and Privacy Act, educational institutions do not have a mandatory breach notification requirement in the same form as HIPAA or GDPR. FERPA prohibits unauthorized disclosure of student education records but does not prescribe a specific breach notification process to a regulator. In practice, institutions that experience a breach involving student records report it to the US Department of Education and notify affected students and parents, in accordance with FERPA guidance and applicable state breach notification laws. Possible FERPA violations are reported to the Family Policy Compliance Office within the Department of Education.
The FDA’s serious breach reporting requirements apply specifically to sponsors and investigators in clinical trials regulated under Good Clinical Practice standards. A serious breach, one that is likely to affect the safety of trial participants or the reliability of trial data, must be reported to the FDA and, in the EU, to the relevant competent authority, typically within 7 to 15 days of the sponsor becoming aware of it. This is a distinct obligation from general data privacy breach reporting and sits within the clinical research regulatory framework rather than consumer privacy law.
For critical infrastructure sectors- energy, financial services, water, transportation- the Cybersecurity and Infrastructure Security Agency coordinates incident reporting under the Cyber Incident Reporting for Critical Infrastructure Act of 2022 (CIRCIA). CIRCIA requires covered entities to report significant cyber incidents to CISA within 72 hours and ransomware payments within 24 hours, with implementing regulations still being finalized as of 2024. Organizations in these sectors may also have parallel reporting obligations to their sector-specific regulators: FERC for energy, banking regulators for financial institutions, and the TSA for transportation.
HIPAA Breach Reporting Requirements
HIPAA breach reporting requirements obligate covered entities and their business associates to notify affected individuals, HHS OCR, and, in some cases, the media whenever protected health information is accessed, used, or disclosed without authorization in a manner that compromises its security or privacy. These requirements are not discretionary; non-compliance carries civil monetary penalties ranging from $100 per violation to $1.9 million per violation category per year, with criminal referrals possible in cases of willful neglect.

The HIPAA Breach Notification Rule, codified at 45 CFR §§ 164.400–414, establishes the full scope of these obligations. It applies to every covered entity, healthcare providers, health plans, and healthcare clearinghouses, and to every business associate that creates, receives, maintains, or transmits PHI on their behalf. Understanding exactly what triggers a reporting obligation, when it must be filed, and how the submission process works is foundational to any HIPAA compliance program.
What Is a Reportable HIPAA Breach?
A reportable HIPAA breach is any impermissible use or disclosure of protected health information that is not otherwise permitted under the Privacy Rule, and that poses a significant risk of financial, reputational, or other harm to the affected individual. The definition is intentionally broad: it covers accidental disclosures, insider misuse, ransomware attacks that encrypt PHI, misdirected emails, lost or stolen devices containing unencrypted records, and unauthorized access by third parties, among many other scenarios.
PHI is defined under HIPAA as individually identifiable health information transmitted or maintained in any form, electronic, paper, or oral, that relates to an individual’s past, present, or future physical or mental health condition, the provision of healthcare, or payment for healthcare. The combination of a name with a diagnosis, a Social Security number with treatment records, or an account number with insurance information all constitute PHI and are subject to the Breach Notification Rule when exposed without authorization.
It is important to understand that a HIPAA breach is not limited to cyberattacks or external intrusions. An employee accessing a patient’s record out of curiosity, a fax sent to the wrong recipient, or a paper record left in an unsecured location can all constitute reportable breaches if the impermissible disclosure meets the harm threshold. The manner in which the breach occurred does not determine whether it is reportable; the nature of what was exposed and the risk it poses to the affected individual does.
Every HIPAA Breach Must Be Reported Unless…
HIPAA establishes a presumption that every impermissible use or disclosure of PHI is a reportable breach. That presumption can only be rebutted, not assumed away, through a documented four-factor risk assessment that demonstrates a low probability that the PHI was compromised. This is one of the most consequential aspects of the Breach Notification Rule: the burden of proof sits entirely with the covered entity or business associate, not with the regulator.
The four factors the risk assessment must evaluate are: the nature and extent of the PHI involved, including the types of identifiers and the likelihood of re-identification; the identity of the unauthorized person who used or accessed the PHI; whether the PHI was actually acquired or viewed, or whether there is a low probability this occurred; and the extent to which the risk to the PHI has been mitigated following the incident.
Beyond the four-factor assessment, HIPAA also carves out three specific categories of impermissible disclosure that are explicitly excluded from the definition of a breach. The first is an unintentional acquisition, access, or use of PHI by a workforce member acting in good faith within their scope of authority, provided the information is not further used or disclosed impermissibly. The second is an inadvertent disclosure by one authorized person to another within the same covered entity or business associate, again with no further impermissible use. The third is a disclosure where the covered entity or business associate has a good-faith belief that the unauthorized recipient could not reasonably have retained the information.
These exclusions are narrow and fact-specific. Organizations that broadly apply them without documentation to avoid notification obligations expose themselves to significant enforcement risk.
HIPAA Breach Reporting to HHS OCR, How to Use the Portal
All HIPAA breach reports to HHS OCR are submitted through the OCR Breach Reporting Portal, accessible at ocrportal.hhs.gov. The portal is the exclusive submission mechanism for covered entities and business associates; there is no paper alternative for electronic submissions, and reports sent by other means will not be accepted as compliant filings.
To submit a breach report, the covered entity or business associate must create an account on the portal if one does not already exist. The submission form requires detailed information about the covered entity, the nature of the breach, the date of discovery, the date of the breach if known, the approximate number of individuals affected, the type of PHI involved, the location of the breached information, and the safeguards in place at the time of the breach. The portal also asks for a description of what the organization has done or plans to do to investigate the breach, mitigate harm, and prevent future occurrences.
For breaches affecting 500 or more individuals, the portal submission triggers immediate public posting on the HHS OCR breach portal, the public-facing database that lists all large HIPAA breaches currently under investigation or resolved within the past 24 months. Covered entities should anticipate that their submission will become publicly visible, and prepare external communications accordingly before filing. For small breaches affecting fewer than 500 individuals, the annual log submission through the portal does not result in public posting by default.
HIPAA Breach Reporting Timeline for Large vs. Small Breaches
HIPAA’s Breach Notification Rule establishes a two-track reporting timeline based on the number of individuals affected, and determining which track applies is one of the first steps a covered entity must take after a breach is discovered.
For breaches affecting 500 or more individuals, covered entities must notify HHS OCR, affected individuals, and, if the breach affects residents of a specific state or jurisdiction, prominent media outlets in that area, all within 60 days of discovering the breach. The 60-day window is a ceiling, not a target. HHS OCR has consistently stated that notification should occur as soon as reasonably possible, and that using the full 60 days as a default delay, rather than completing notification as soon as the investigation allows, is inconsistent with the spirit and intent of the rule.
For breaches affecting fewer than 500 individuals, covered entities must still notify affected individuals within 60 days of discovery. The distinction for small breaches is in the HHS OCR reporting pathway: rather than an immediate portal submission, the covered entity logs the breach and submits it through the portal as part of an annual report, due within 60 days after the end of the calendar year in which the breach occurred. This means a small breach discovered in January could be reported to HHS OCR as late as March 1 of the following year. However, individual notification is still due within 60 days of the January discovery date.
Business associates must report breaches to the covered entity within 60 days of discovery, though business associate agreements routinely shorten this window to 10 or 30 days. The covered entity’s reporting timeline to HHS OCR and affected individuals runs from the date the covered entity discovered or should have discovered the breach, which, if the business associate delayed notification, can create a compliance gap the covered entity is responsible for bridging.
Notifying Affected Individuals Under HIPAA
HIPAA requires that notice to affected individuals be written in plain language and delivered by first-class mail to the individual’s last known address, or by email if the individual has agreed to receive communications electronically, and that agreement has not been withdrawn. The notice must contain four core elements: a brief description of what happened, including the date of the breach and the date of discovery; a description of the types of PHI involved; the steps individuals should take to protect themselves from potential harm; a brief description of what the covered entity is doing to investigate and mitigate the breach and prevent future occurrences; and contact information for individuals to ask questions or obtain additional information.
When a covered entity lacks sufficient contact information for 10 or more individuals, substitute notice is required. For those individuals, the covered entity must either post a conspicuous notice on its website for 90 days or provide notice to major print or broadcast media in the geographic areas where the affected individuals are likely to reside. A toll-free phone number that remains active for at least 90 days must be included in the substitute notice, giving individuals a direct channel to inquire whether their information was involved in the breach.
For breaches affecting 500 or more residents of a specific state or jurisdiction, media notification is required in addition to individual notice, not as a substitute for it. The media notice must go to prominent outlets in the relevant area within the same 60-day window that governs the HHS OCR submission and individual notifications.
HIPAA Breach Reporting Form and Submission Process
The HIPAA breach reporting form is embedded within the HHS OCR portal at ocrportal.hhs.gov and must be completed digitally; there is no standalone downloadable form for submitting large breach reports. The portal walks covered entities through a structured intake process that sequentially covers all required disclosure elements.
The information the form requires includes: the name, address, and contact information of the covered entity; the type of covered entity; the date the breach was discovered and, if known, the date it occurred; the approximate number of individuals whose PHI was involved; the type of breach, such as hacking, unauthorized access, theft, loss, or improper disposal; the location of the breached PHI, electronic medical records, paper records, portable devices, email systems, and so on; the type of PHI involved, demographic data, financial information, clinical information, and so on; and a narrative description of the breach and the response measures taken.
Before submitting, covered entities should ensure that their breach risk assessment is fully documented and retained, that individual notification has been prepared and is ready for simultaneous release, and that any media notification requirements have been assessed. The portal submission is not the end of the compliance process; HHS OCR may open an investigation following any large breach submission, request additional documentation, and, in cases where systemic compliance failures are identified, initiate formal enforcement proceedings. Maintaining a complete breach response file, including the risk assessment, notification records, and internal communications, is essential preparation for that possibility.
GDPR Data Breach Reporting Requirements
GDPR data breach reporting requirements obligate data controllers to notify their supervisory authority within 72 hours of becoming aware of a personal data breach, and to notify affected individuals without undue delay when that breach is likely to result in a high risk to their rights and freedoms. These obligations apply to any organization, regardless of its headquarters, that processes the personal data of individuals in the European Union.

The GDPR’s breach notification framework is established under Articles 33 and 34 of the regulation, and it represents one of the most demanding breach disclosure regimes in global privacy law. Unlike regulatory frameworks that focus primarily on sensitive data categories, GDPR’s notification obligation can be triggered by a breach involving any personal data, such as names, email addresses, IP addresses, or location data, provided the breach creates a meaningful risk of harm. The European Data Protection Board’s Guidelines 01/2021 on Examples of Personal Data Breach Notification provide the most detailed practical guidance on how supervisory authorities expect these obligations to be applied.
The 72-Hour Rule Under GDPR, What It Means in Practice
The 72-hour rule under GDPR requires data controllers to notify their lead supervisory authority within 72 hours of becoming aware that a personal data breach has occurred, not within 72 hours of confirming every detail of the breach, and not within 72 hours of completing an internal investigation. The clock starts at awareness, and it does not pause for investigation, legal review, or executive sign-off.
In practice, this means organizations need incident detection and internal escalation processes that are fast enough to deliver a credible initial assessment to a privacy officer or DPO within hours of a breach being identified, not days. The EDPB’s guidance acknowledges that organizations will rarely have complete information within 72 hours, and explicitly permits phased notification: an initial report filed within the deadline with the information available at the time, followed by supplementary filings as the investigation develops. What the regulation does not permit is using investigative incompleteness as a reason to delay filing the initial notification.
The 72-hour window is calculated in calendar hours, not business hours. A breach discovered at 11 pm on a Friday triggers a deadline of 11 pm on Monday, regardless of whether the supervisory authority’s offices are open. Organizations that limit breach response to business hours will routinely miss the deadline. This is one of the most operationally significant aspects of the rule, and it is the reason that effective GDPR compliance requires a 24/7 incident response capability, or at minimum a clear escalation protocol that functions outside normal working hours.
When a controller fails to meet the 72-hour deadline, GDPR requires the notification to be filed as soon as possible, accompanied by a reasoned explanation for the delay. Supervisory authorities across the EU have made clear that reasons such as “we were still investigating” or “we were waiting for legal advice” are not automatically accepted as valid justifications. Repeated or systemic delays have led to enforcement action independent of the breach itself.
Reporting a Data Breach to Your DPA
Under GDPR, data controllers report personal data breaches to their lead supervisory authority, the Data Protection Authority of the EU member state in which the controller has its main establishment, defined as the place of its central administration in the EU. For organizations with establishments in multiple EU member states, the lead DPA is determined by where the controller’s central decision-making about data processing activities takes place.
Each EU member state’s DPA operates its own breach notification portal or submission process. In Ireland, for example, the Data Protection Commission receives breach notifications through its online portal. In Germany, notifications go to the relevant Landesbeauftragter für den Datenschutz (state-level DPA), depending on where the controller is established, since Germany’s DPA structure is federal rather than centralized. In France, notifications go to the CNIL. Controllers operating in the EU must identify their lead DPA before a breach occurs and ensure their incident response procedures are mapped to that authority’s specific submission format and requirements.
The notification must contain, at minimum: the nature of the breach, including the categories and approximate number of individuals and personal data records involved; the name and contact details of the data protection officer or other point of contact; the likely consequences of the breach; and the measures taken or proposed to address the breach and mitigate its effects. If all of this information is not available within 72 hours, the controller submits what is known and provides a timetable for when further information will be available. The EDPB has confirmed that supervisory authorities prefer early, incomplete notifications to late, complete ones.
When Do You Need to Notify Data Subjects Under GDPR?
Notification to affected data subjects under GDPR is required when a breach is likely to result in a high risk to the rights and freedoms of natural persons. This is a higher threshold than the one that triggers a supervisory authority notification; not every breach that must be reported to a DPA also requires direct notification to the affected individuals.
A high risk to rights and freedoms means there is a significant probability that the breach will lead to physical, material, or non-material harm to the individuals whose data was involved. The EDPB identifies the following as indicators of high risk: identity theft or fraud, financial loss, damage to reputation, loss of confidentiality of data subject to professional secrecy, unauthorized reversal of pseudonymization, significant economic or social disadvantage, and any other substantial adverse effect on the individual. The more sensitive the data involved- health records, financial credentials, biometric data, data relating to children- the more likely the high-risk threshold is met.
When the high-risk threshold is met, notification to data subjects must be provided without undue delay; no fixed number of hours is specified for individual notification. Still, supervisory authorities expect it to follow the DPA notification closely, and any unreasonable delay will be scrutinized. The notice must communicate the nature of the breach, the contact details of the DPO or responsible contact, the likely consequences of the breach, and the measures taken or recommended to mitigate potential harm. It must be written in clear, plain language; legal boilerplate that obscures the practical implications for the individual is not compliant.
GDPR provides three circumstances in which individual notification can be waived even when a high-risk breach has occurred: where the controller has implemented appropriate technical measures, such as strong encryption, that render the data unintelligible to anyone who accessed it; where the controller has taken subsequent measures that ensure the high risk to data subjects is no longer likely to materialize; or where individual notification would involve disproportionate effort, in which case a public communication or equivalent measure must be used instead. Supervisory authorities assess these exemptions strictly, and controllers relying on them should retain detailed documentation of the technical measures and the reasoning behind them.
GDPR Breach Reporting When You’re a Processor vs. Controller
The GDPR’s breach notification obligations fall primarily on data controllers, the entities that determine the purposes and means of processing personal data. Data processors, entities that process personal data on behalf of a controller, carry a different, but equally important, obligation that feeds directly into the controller’s ability to meet its own deadlines.
Under Article 33(2), a processor that becomes aware of a personal data breach must notify the controller without undue delay. There is no 72-hour window specified for processor-to-controller notification; the phrase “without undue delay” sets the standard, and the EDPB’s guidance makes clear that this should be interpreted as immediate or as close to immediate as the circumstances permit. The urgency stems from a structural factor: the controller’s 72-hour clock to the DPA begins when it becomes aware of the breach, typically when the processor notifies it. Every hour the processor delays is an hour consumed from the controller’s regulatory deadline.
Contracts between controllers and processors, the Data Processing Agreements required under Article 28, typically specify a contractual notification deadline shorter than the one the GDPR prescribes. Deadlines of 24 hours or even 12 hours from processor discovery to controller notification are common in well-drafted DPAs, precisely because giving the controller maximum time to conduct its own assessment and meet the 72-hour window is in both parties’ interest.
Processors do not submit breach notifications directly to supervisory authorities; that obligation belongs exclusively to the controller. However, processors are required to assist controllers in meeting their notification obligations, which in practice means providing all relevant technical information about the breach, cooperating with the controller’s investigation, and making relevant personnel available to answer regulator questions if the controller’s DPA notification triggers an inquiry.
ICO Personal Data Breach Reporting, 72-Hour Guidance
The Information Commissioner’s Office is the UK’s data protection regulator and the supervisory authority for UK GDPR breach notifications following Brexit. UK GDPR mirrors the EU regulation’s 72-hour notification requirement, and the ICO has published detailed guidance, including a self-assessment tool and worked examples, to help organizations determine whether a breach is notifiable and how to file a compliant report.
The ICO’s breach reporting portal is at ico.org.uk/make-a-complaint/data-security-breach-report. Organizations must report breaches that are likely to result in a risk to individuals’ rights and freedoms, the same threshold as EU GDPR. The ICO has stated publicly that it receives thousands of breach reports annually and uses a risk-based approach to prioritize which to investigate further, but that being selected for investigation does not depend solely on breach severity; late, inadequate, or poor-quality notifications increase the likelihood of regulatory scrutiny.
The ICO’s guidance on the 72-hour window addresses several practically important scenarios. If an organization receives a credible report of a breach from an external source, a journalist, a third party, or a customer, and cannot immediately confirm or deny it, the ICO considers this a point of awareness that starts the clock. Organizations cannot avoid the 72-hour deadline by treating unconfirmed reports as outside the scope of notification obligations until internal verification is complete. The ICO expects organizations to begin their notification process based on reasonable belief, even while investigation continues.
The ICO also emphasizes that the quality of the initial notification matters. Reports that contain only minimal information, such as “we may have experienced a breach” with no description of the data or individuals involved, are treated as inadequate, even if they are technically filed within 72 hours. The ICO expects organizations to provide the best available information at the time of filing and to supplement it promptly as the investigation progresses.
Reporting a GDPR Breach Anonymously or Internationally
GDPR does not provide a mechanism for anonymous breach reporting to a supervisory authority. Article 33 requires that the notification include the name and contact details of the data protection officer or other point of contact; anonymity is structurally incompatible with the regulation’s accountability framework, which is built on the premise that the supervisory authority can follow up with the controller to request additional information, assess the response, and, if necessary, open an enforcement investigation.
This means organizations cannot report a GDPR breach to a DPA without identifying themselves, and individuals cannot file a GDPR breach notification on behalf of an organization. A data subject who believes their personal data has been breached can report their concern to their national DPA, which may then investigate the relevant controller, but this is a complaint mechanism, not a breach notification pathway.
For organizations operating internationally, particularly those with data subjects in both EU and non-EU jurisdictions, GDPR breach reporting runs parallel to, rather than replacing, other jurisdictional obligations. A breach affecting EU and US data subjects simultaneously triggers the GDPR’s 72-hour DPA notification requirement and the applicable US federal or state obligations for US data. These obligations are independent and must both be satisfied. The EDPB’s one-stop-shop mechanism means that a controller with a single EU lead DPA can file one GDPR notification with that lead authority, which then coordinates with other concerned EU supervisory authorities, but this applies only within the EU framework and does not reduce obligations under other jurisdictions’ laws.
Organizations subject to both GDPR and the UK GDPR, those with establishments or data subjects in both the EU and the UK, must notify both their EU lead DPA and the ICO when a breach affects individuals in both territories. Brexit created a dual-filing requirement that did not exist when the UK was an EU member state, and organizations that have not updated their breach response procedures to reflect this should treat it as a gap requiring immediate remediation.
Data Breach Reporting Requirements by Jurisdiction
Data breach reporting requirements vary significantly by jurisdiction; there is no single global standard, and most organizations operating across borders face overlapping obligations under multiple frameworks simultaneously. Where you are established, where your customers are located, and what type of data was compromised all determine which laws apply and which authorities must be notified.

The practical consequence of this jurisdictional complexity is that a single breach can trigger parallel notification obligations across federal regulators, state attorneys general, international supervisory authorities, and sector-specific bodies, each with different timelines, thresholds, and submission formats. Organizations that map these obligations in advance, rather than during an active incident, are substantially better positioned to meet every deadline without compounding a breach into a compliance failure.
US Federal Requirements (SEC, FCC, FERPA, HIPAA, CCPA, PCI)
The United States does not have a single federal data breach notification law. Instead, breach reporting obligations at the federal level are distributed across a set of sector-specific and issue-specific regulations, each governing a defined category of data or a defined class of organization. Understanding which federal frameworks apply to your organization, and how they interact, is the foundation of any US breach response plan.
HIPAA governs breaches of protected health information held by covered entities and their business associates, requiring notification to HHS OCR, affected individuals, and in some cases media outlets within 60 days of discovery. The SEC’s cybersecurity disclosure rules, effective December 2023, require publicly traded companies to report material cybersecurity incidents via Form 8-K within four business days of determining materiality. The FCC’s updated breach reporting rules require telecommunications carriers to notify the FBI, the Secret Service, and the FCC within 7 business days of determining that a breach of Customer Proprietary Network Information has occurred, with customer notification to follow.
FERPA governs student education records at federally funded educational institutions. Unlike HIPAA and the SEC rules, FERPA does not prescribe a specific breach notification timeline or mandatory reporting pathway to a federal regulator; institutions are expected to notify affected students and parents under a combination of FERPA guidance and applicable state law. Complaints about FERPA violations are directed to the Family Policy Compliance Office within the US Department of Education.
The Payment Card Industry Data Security Standard, PCI DSS, is a contractual framework rather than a law. Still, its breach notification requirements carry significant practical force for any organization that accepts, processes, or stores payment card data. Organizations that experience a breach involving cardholder data must notify their acquiring bank and the relevant card brands, Visa, Mastercard, American Express, and Discover, immediately upon suspecting a breach, often within 24 hours. The card brands then conduct their own forensic investigations, which are entirely separate from any regulatory notification obligation.
CCPA, as amended by the CPRA, applies to for-profit businesses that meet defined revenue or data volume thresholds and collect personal information from California residents. It does not impose a fixed notification deadline in hours or days. Still, it requires notification as soon as possible and without unreasonable delay, with enforcement by the California Attorney General and a private right of action for affected individuals.
Data Breach Reporting Requirements by State
Every US state, the District of Columbia, Puerto Rico, Guam, and the US Virgin Islands have enacted a data breach notification law, creating a patchwork of requirements that any organization handling personal information about US residents must navigate. According to the Identity Theft Resource Center, the number of data compromises reported in the United States reached 3,205 in 2023, a record high, making state-level compliance more operationally consequential than ever.
The core elements that vary across state breach laws are: the definition of personal information that triggers notification, the notification deadline, who must be notified beyond affected individuals, and the required content of the notification. Most state laws define personal information as a combination of a name with a Social Security number, financial account number, driver’s license number, or similar government-issued identifier. An expanding group of states, including California, Colorado, Virginia, Connecticut, and New York, have extended their definitions to include health data, biometric identifiers, login credentials, precise geolocation, and genetic information.
Notification deadlines range from as few as 30 days after discovery, in states including Florida, Ohio, and Washington, to the more common standard of “in the most expedient time possible without unreasonable delay,” which courts and regulators have generally interpreted to mean 30 to 45 days in practice. New York’s SHIELD Act requires notification to the affected individuals, the New York Attorney General, the Department of State, and the Division of State Police for breaches affecting New York residents. California’s law requires notification to the California Attorney General when a breach affects more than 500 California residents. Texas requires businesses to notify the Texas Attorney General of breaches affecting 250 or more Texas residents within 30 days.
Organizations operating nationally must assess each breach against the most expansive state law applicable to any resident whose data was involved, not just the law of the state where the organization is headquartered. A breach affecting residents in 20 states may trigger 20 simultaneous, partially inconsistent notification obligations, each requiring individual tracking and documented compliance.
UK Data Breach Reporting (UK GDPR / ICO)
Following the United Kingdom’s exit from the European Union, the UK enacted its own version of the General Data Protection Regulation, UK GDPR, which came into force on January 1, 2021. UK GDPR retains the core structure and obligations of EU GDPR, including the 72-hour breach notification requirement, but operates as an independent legal framework enforced by the Information Commissioner’s Office rather than an EU supervisory authority.
Under UK GDPR, data controllers must report personal data breaches that are likely to result in a risk to individuals’ rights and freedoms to the ICO within 72 hours of becoming aware of the breach. The notification is submitted through the ICO’s online breach reporting portal. As with EU GDPR, the 72-hour window is a filing deadline for the initial notification, not a deadline for completing the investigation, and controllers are permitted to supplement initial reports with additional information as it becomes available.
The ICO’s enforcement posture has become increasingly assertive. The ICO has issued fines under UK GDPR for late notification, inadequate security measures that enabled breaches, and failure to notify affected individuals when the high-risk threshold was met. The maximum fine under UK GDPR is £17.5 million or 4 percent of global annual turnover, whichever is higher, the same proportional ceiling as EU GDPR, translated into sterling.
Organizations subject to both the EU GDPR and the UK GDPR, and those processing personal data of individuals in both the EU and the UK, must notify both their EU lead DPA and the ICO when a breach affects individuals in both territories. Brexit effectively created a dual-filing requirement that did not exist before January 2021, and organizations that have not updated their breach response procedures to reflect this should treat it as a live compliance gap.
Canada, PIPEDA Mandatory Breach Reporting
Canada’s mandatory breach reporting regime is established under the Personal Information Protection and Electronic Documents Act, as amended by the Digital Privacy Act in 2018. PIPEDA applies to private-sector organizations that collect, use, or disclose personal information in the course of commercial activities, covering a wide range of businesses operating in federally regulated sectors and across provincial borders.
The central concept governing PIPEDA breach reporting is real risk of significant harm. Unlike GDPR, which requires notification to the supervisory authority for any breach that poses a risk to rights and freedoms, PIPEDA’s reporting threshold is higher: notification to both the Office of the Privacy Commissioner of Canada and affected individuals is required only when a breach creates a real risk of significant harm to an individual. Significant harm is defined to include bodily harm, humiliation, damage to reputation or relationships, financial loss, identity theft, negative effects on a credit record, and damage to or loss of employment or professional opportunities.
When the real risk of significant harm threshold is met, organizations must notify the OPC and affected individuals as soon as feasible; there is no fixed number of hours or days prescribed by the statute. The OPC’s guidance interprets “as soon as feasible” to mean promptly after the determination is made, and it does not accept extended delays for investigative purposes as a valid justification. The notification to the OPC must include a description of the breach, the personal information involved, the number of individuals affected, steps taken to reduce the risk of harm, and steps taken to notify affected individuals.
Critically, PIPEDA requires organizations to maintain a record of every breach of security safeguards, regardless of whether the breach meets the reporting threshold, for a minimum of 24 months from the date the organization determined the breach occurred. The OPC can request access to these records at any time, and failure to maintain them is itself a violation independent of the underlying breach. Alberta, British Columbia, and Quebec have their own substantially similar provincial privacy laws that apply to organizations operating within those provinces, with Quebec’s Law 25, updated in 2023, introducing some of the strictest breach notification requirements in Canada.
Australia, OAIC Notifiable Data Breaches Scheme
Australia’s Notifiable Data Breaches scheme, which came into effect in February 2018 under Part IIIC of the Privacy Act 1988, requires organizations covered by the Privacy Act to notify the Office of the Australian Information Commissioner and affected individuals when an eligible data breach occurs. The scheme applies to Australian Government agencies, businesses, and not-for-profit organizations with an annual turnover of more than AU$3 million, and to certain other organizations, regardless of turnover, including health service providers, credit reporting bodies, and tax file number recipients.
An eligible data breach under the NDB scheme involves unauthorized access to or disclosure of personal information, or loss of personal information where unauthorized access or disclosure is likely. It is likely to result in serious harm to one or more of the individuals whose information was involved. Serious harm is assessed against a set of factors specified in the Privacy Act, including the sensitivity of the information, whether it was protected by security measures, the likelihood and nature of harm if it were misused, and the persons who accessed or are likely to access it.
If an organization suspects an eligible data breach may have occurred but is not certain, it has 30 days to conduct an assessment. That assessment period is itself a regulatory deadline; organizations cannot conduct an indefinite investigation to delay the notification obligation. If the assessment concludes that an eligible data breach has occurred, notification to the OAIC and affected individuals must happen as soon as practicable. If direct notification to all affected individuals is not reasonably practicable, the organization must publish a statement on its website and take reasonable steps to publicize it.
Following the Optus and Medibank breaches in 2022, which collectively affected tens of millions of Australians, the Australian government significantly increased maximum penalties for serious or repeated privacy breaches to AU$50 million, three times the value of any benefit obtained through the misuse of information, or 30 percent of adjusted domestic turnover for the relevant period, whichever is greatest. The Privacy Act is also currently undergoing its most significant reform in decades, with proposed amendments expected to introduce direct rights of action for individuals and expanded OAIC enforcement powers.
ASIC Breach Reporting (RG 78)
The Australian Securities and Investments Commission administers a separate breach reporting regime that applies to Australian financial services licensees and Australian credit licensees, covering banks, insurers, superannuation funds, financial advisers, mortgage brokers, and other entities operating under an AFS or credit licence. This regime is governed by ASIC Regulatory Guide 78 and operates alongside, not instead of, the OAIC’s NDB scheme for breaches involving personal information.
Under the Corporations Act 2001, as amended by the Financial Sector Reform (Hayne Royal Commission Response) Act 2020, AFS licensees and credit licensees are required to report significant breaches, or likely significant breaches, of their licence obligations to ASIC within 30 calendar days of becoming aware of the breach. A breach is significant if it meets one or more criteria: it results from conduct that is systemic or involves multiple instances; it results in, or is likely to result in, material loss or damage to clients; it involves serious fraud; or it is otherwise of a kind prescribed by the regulations.
The 30-day reporting deadline runs from the date the licensee becomes aware that a significant breach has occurred or is likely to have occurred, not from the date of the breach itself. ASIC has emphasized that licensees should have internal systems capable of identifying and escalating potential breaches quickly, since delays in internal identification that push reporting past 30 days are treated as compliance failures regardless of the cause. ASIC receives the breach report through its online portal and may investigate the licensee’s conduct, systems, and internal controls in response.
Financial services licensees subject to both ASIC’s regime and the OAIC’s NDB scheme, which in practice means most licensees handling customer personal information, must assess each incident under both frameworks and satisfy whichever obligations are triggered. The ASIC breach and the notifiable data breach may arise from the same incident but require separate notifications to different regulators, with different timelines and content requirements. Coordinating these parallel filings without creating conflicting public statements is one of the more operationally demanding aspects of breach response for Australian financial institutions.
How to Report a Data Breach, Step by Step
Reporting a data breach correctly requires following a defined sequence of actions: containment, assessment, authority identification, notification, individual communication, and documentation, in the right order and within legally mandated timeframes. Skipping or reordering these steps is one of the most common ways organizations compound a breach into a compliance failure.

The process below applies regardless of which regulation governs the breach. The specific deadlines, authorities, and form requirements vary by jurisdiction, but the operational sequence is consistent across HIPAA, GDPR, CCPA, PIPEDA, and other major frameworks.
Step 1: Contain the Breach
The first action following discovery of a data breach is containment, stopping the unauthorized access, disclosure, or loss from continuing or expanding before any assessment or notification work begins. Containment measures depend on the nature of the breach: isolating compromised systems from the network, revoking unauthorized access credentials, recovering lost or stolen devices, halting a misdirected data transfer, or turning off a vulnerable application endpoint.
Containment does not mean remediation. Organizations frequently make the mistake of attempting full remediation, patching vulnerabilities, rebuilding systems, restoring from backups, before preserving the forensic evidence needed to assess the breach’s scope and cause. Effective containment stops the bleeding while preserving the evidence. Forensic preservation should run in parallel with containment, not after it.
Speed matters at this stage beyond the obvious operational reasons. In most jurisdictions, the regulatory reporting clock begins when the organization becomes aware of the breach, not when containment is complete. Every hour spent on containment is an hour consumed from the notification deadline. Containment and initial incident assessment must happen simultaneously, not sequentially.
Step 2: Assess Scope and Determine Reportability
Once the breach is contained, the organization must conduct a structured assessment to determine what data was involved, how many individuals are affected, whether the data was actually accessed or merely at risk, and whether the incident meets the legal definition of a reportable breach under the applicable regulation or regulations.
This assessment is not optional, and its conclusions must be documented. Under HIPAA, a four-factor risk assessment is the mechanism by which a covered entity can rebut the presumption that a breach is reportable; without it, every impermissible PHI disclosure is presumed notifiable. Under GDPR, the controller must assess whether the breach is likely to result in a risk to individuals’ rights and freedoms before determining whether DPA notification is required, and whether the risk is high enough also to require individual notification. Under PIPEDA, the determination of real risk of significant harm is the gateway to the entire reporting obligation.
The assessment should identify the categories of data involved, names, financial credentials, health records, government identifiers, login credentials, the approximate number of individuals affected, the timeframe of the exposure, and whether any technical safeguards such as encryption meaningfully limited the harm potential. Organizations operating under multiple regulations should assess reportability under each framework in parallel, as different thresholds can yield different notification obligations for the same incident.
Step 3: Identify the Correct Reporting Authority
With the reportability determination made, the next step is to identify every authority that must be notified and the applicable deadline for each. This means mapping the breach against every regulatory framework that governs the data involved and the jurisdictions where affected individuals reside, not just the framework most familiar to the organization’s compliance team.
A single breach can trigger simultaneous obligations to the ICO under UK GDPR, a lead DPA under EU GDPR, HHS OCR under HIPAA, the SEC if the organization is publicly traded, state attorneys general under applicable US state laws, and the OPC under PIPEDA if Canadian residents are affected. Each of these authorities has a different deadline, a different submission portal, and different minimum content requirements for the initial notification. Failing to identify one of these obligations before the deadline passes is treated by regulators as non-compliance, regardless of whether the other notifications were filed correctly.
This step is where pre-incident preparation has the greatest impact. Organizations that have mapped their regulatory obligations, identified the relevant reporting portals, and designated the personnel responsible for each submission before a breach occurs will complete this step in hours rather than days.
Step 4, File Notification Within the Required Timeframe
Regulatory notification must be filed within the timeframe prescribed by each applicable regulation, using the submission format required by the authority. Under the EU and UK GDPR, this means a structured online submission to the relevant DPA within 72 hours of becoming aware. For HIPAA large breaches, it means a portal submission to HHS OCR within 60 days of discovery. For the SEC, it means filing a Form 8-K within 4 business days of a materiality determination. For US-CERT under DOD requirements, it means a notification within one hour of discovery.
Where complete information is not available within the required timeframe, which is almost always the case under the 72-hour GDPR window, organizations should file an initial notification with the information available and clearly indicate that supplementary information will follow. Most supervisory authorities explicitly accommodate phased reporting, and an incomplete but timely notification is treated far more favorably than a complete but late one.
The notification should be filed by the designated privacy officer, DPO, legal counsel, or incident response lead, whoever has been assigned responsibility in the organization’s incident response plan. Submissions should be saved, timestamped, and retained in the breach documentation file, along with any confirmation or reference number provided by the reporting portal.
Step 5: Notify Affected Individuals
Individual notification is a separate obligation from regulator notification, triggered by a different threshold under most frameworks, and subject to its own content requirements and delivery standards. Under GDPR, it is required when a breach poses a high risk to individuals’ rights and freedoms. Under HIPAA, every reportable breach must be reported and must reach affected individuals within 60 days of discovery. Under CCPA and most US state laws, individual notification is required as soon as reasonably practicable following a qualifying breach.
The notice to affected individuals must be written in plain language, not legal boilerplate. It must explain what happened, which data were involved, what the individual can do to protect themselves, and how to contact the organization for more information. Most regulations also require the notice to describe what the organization has done or is doing to address the breach and prevent recurrence.
Delivery is typically by first-class mail or email, depending on the regulations and the individual’s recorded communication preferences. When contact information is insufficient to reach a meaningful number of affected individuals, ten or more under HIPAA, for example, substitute notice mechanisms apply: website posting, media notice, or public announcement, depending on the jurisdiction. Organizations should prepare individual notification letters in parallel with the regulatory filing process, so both can be deployed as soon as the relevant threshold determinations are complete.
Step 6: Document Everything and Maintain Audit-Ready Records
Every step of the breach response process must be documented contemporaneously and retained in a format that can be produced to regulators on request. Documentation requirements exist under every major framework: GDPR’s accountability principle requires controllers to demonstrate compliance with notification obligations; HIPAA requires covered entities to retain breach documentation for 6 years; PIPEDA requires a breach record for every incident, whether or not it meets the reporting threshold, for a minimum of 24 months.
The breach documentation file should include the initial incident report, the containment log, the risk assessment and reportability determination with supporting reasoning, copies of all regulatory notifications with submission timestamps, copies of individual notices with proof of delivery, any communications with law enforcement, and a post-incident review summarizing lessons learned and remediation actions taken.
This documentation serves two distinct purposes. It demonstrates regulatory compliance during an investigation or audit, which can be the difference between a reprimand and a fine. It also serves as institutional memory that informs future incident response. Organizations that document their breaches thoroughly tend to respond to subsequent incidents more effectively because they have a reference point for what worked and what didn’t.
Failure to Report a Data Breach, Penalties and Consequences
Failing to report a data breach on time, or failing to report it at all, is treated by regulators as a standalone compliance violation, independent of the breach itself, and is subject to its own penalties. The financial consequences range from significant to existential depending on the regulation, the jurisdiction, and whether the failure was inadvertent or willful.
Under GDPR, fines for breaches of notification requirements can reach €10 million or 2 percent of global annual turnover, whichever is higher. The EU’s supervisory authorities have issued fines in this category against organizations that discovered breaches, delayed notification while investigating, and ultimately failed to meet the 72-hour window. Under HIPAA, civil monetary penalties for breach notification failures range from $100 to $50,000 per violation, with annual caps reaching $1.9 million per violation category, and the Department of Justice can pursue criminal charges in cases of willful neglect. The ICO has issued fines under the UK GDPR for late and inadequate notification, separate from any fine related to the security failure that caused the breach.
Beyond financial penalties, the reputational consequences of delayed or inadequate breach reporting are often more damaging than the fine itself. Regulators in the UK, EU, and Australia routinely publish enforcement decisions, naming the organization, describing the breach, and detailing the notification failures. This public record is permanent and searchable, and for organizations in regulated industries, it can trigger downstream consequences including loss of operating licences, client contract terminations, and increased regulatory scrutiny across all compliance programs.
Data Breach Incident Report, Templates and Forms
A data breach incident report is the formal internal document that captures everything an organization knows about a breach, what happened, what data was affected, who is at risk, and what the organization did in response. It serves as both the foundation for regulatory notifications and the audit-ready record that demonstrates compliance if a regulator investigates.

Having a pre-built incident report template in place before a breach occurs is one of the most operationally valuable things a compliance team can do. When a breach is actively unfolding, the ability to populate a structured document rather than build one from scratch under pressure directly improves the speed and accuracy of the regulatory filings that follow.
What to Include in a Data Breach Incident Report
A complete data breach incident report covers six core areas that regulators across every major framework expect to see documented: the nature and cause of the breach, the data categories and individuals affected, the timeline from occurrence to discovery to containment, the risk assessment and reportability determination, the notification actions taken, and the remediation and prevention measures implemented.
Under the nature and cause section, the report should describe how the breach occurred, whether through external attack, insider misuse, accidental disclosure, lost or stolen device, or system misconfiguration, and identify the specific vulnerability or failure that enabled it. Under data categories, the report should specify the types of personal information involved, the approximate number of records, and the approximate number of individuals. The timeline section should record the date and time the breach occurred (if known), the date and time it was discovered, who discovered it, how it was discovered, and each subsequent action taken with timestamps.
The risk assessment section is particularly important because it is the document regulators will scrutinize most closely during an investigation. It should capture the four-factor HIPAA analysis or the GDPR risk-to-rights-and-freedoms assessment, or both, if multiple frameworks apply, and include the reasoning behind the reportability conclusion, not just the conclusion itself. Supporting evidence, such as encryption status of the compromised data or access logs showing whether the data was actually viewed, should be attached or referenced.
Data Breach Report Template (Free Download)
A standard data breach report template should be structured to capture all required information in a format that can be adapted for both internal documentation and regulatory submission. The template below covers the core elements required under HIPAA, GDPR, CCPA, and PIPEDA. Organizations should adapt it to include any jurisdiction-specific fields required by their applicable regulations.
- Incident Summary: Date and time of discovery, date and time of occurrence (if known), name and role of the person who discovered the breach, brief description of the incident.
- Data Involved: Categories of personal data affected (health records, financial information, login credentials, government identifiers, etc.), approximate number of records, approximate number of individuals, whether the data was encrypted or pseudonymized at the time of the breach.
- Cause and Vector: How the breach occurred (phishing, ransomware, insider access, misconfiguration, lost device, etc.), the specific system or process that failed, and whether the vulnerability has been remediated.
- Risk Assessment: Probability that data was actually accessed or acquired by an unauthorized party, potential harm to affected individuals, applicable regulatory framework(s), reportability determination with supporting reasoning.
- Notification Log: Date and method of regulatory notification for each applicable authority, date and method of individual notification, substitute notice actions taken if direct notification was not practicable, media notice if applicable.
- Remediation Actions: Immediate containment measures taken, longer-term technical and organizational measures implemented or planned to prevent recurrence, third-party forensic investigation engaged (if applicable).
- Sign-Off: Name, title, and signature of the privacy officer, DPO, or designated incident response lead responsible for the report, with date of completion.
Data Breach Reporting Form Requirements by Regulation
Each major data breach regulation specifies minimum content requirements for the formal notification submitted to the relevant authority, and these requirements vary enough that organizations subject to multiple frameworks need to prepare separate submissions rather than a single document adapted for each portal.
GDPR and UK GDPR require the DPA notification to include: the nature of the breach including categories and approximate numbers of data subjects and records involved; the name and contact details of the DPO or other contact point; the likely consequences of the breach; and the measures taken or proposed to address the breach. EU GDPR submissions go through each member state’s DPA portal; UK GDPR submissions go through the ICO’s online portal.
HIPAA requires the HHS OCR portal submission to include: the type of breach, the location of the breached PHI, the type of PHI involved, the date of the breach, the date of discovery, the number of individuals affected, and a description of what happened, what the covered entity is doing to investigate and mitigate the breach, and what steps affected individuals should take.
PIPEDA requires the OPC notification to include: a description of the breach, the personal information involved, the number of individuals affected, the steps taken to reduce risk of harm, and the steps taken or planned to notify affected individuals. CCPA does not prescribe a specific form for the California AG notification, but the AG’s office has published guidance on the information it expects to receive.
Security Breach Incident Report Template
A security breach incident report differs from a privacy-focused data breach report in that it leads with the technical details of the security event, the attack vector, compromised systems, indicators of compromise, and containment timeline, before moving to the personal data and regulatory implications. Security operations teams most commonly use this format to document the incident from a technical perspective, with the privacy officer or legal team then using the security report as input for the regulatory notification.
The security breach incident report should open with an executive summary: a single paragraph that describes what happened, when it was discovered, which systems were affected, and the current status. This summary is the section most likely to be read by executives and board members who need a quick situational picture without technical depth.
The technical body of the report should cover: the attack timeline reconstructed from system logs and forensic analysis, the specific systems and data stores accessed or affected, the indicators of compromise identified during investigation, the containment and eradication actions taken and their timestamps, and the results of any forensic investigation including whether data was exfiltrated, corrupted, or destroyed. A separate section should address the personal data implications, cross-referencing the compromised systems against their data inventories to identify what categories of personal information were at risk and whether the breach meets the regulatory definition of a reportable event.
HIPAA Breach Incident Report Form
HIPAA does not publish a standalone downloadable breach incident report form for covered entities to complete. The formal submission to HHS OCR is made through the structured intake form embedded in the OCR Breach Reporting Portal at ocrportal.hhs.gov. However, covered entities typically maintain an internal breach incident report as a separate document that supports the portal submission and serves as the primary audit-ready record of the incident.
The internal HIPAA breach incident report should document: the name and contact information of the covered entity; the identity of the business associate involved, if applicable; the date the breach was discovered and the date it occurred if known; a description of the impermissible use or disclosure; the type and number of individuals affected; the type of PHI involved; the four-factor risk assessment with supporting evidence and conclusions; the notification actions taken, including dates of individual notification, HHS OCR submission, and any media notice; and the safeguards that were in place at the time of the breach and any additional safeguards implemented in response.
This internal document should be retained for a minimum of six years from the date of its creation or the date it was last in effect, whichever is later, consistent with HIPAA’s documentation retention requirements. HHS OCR investigators routinely request internal breach documentation during compliance reviews, and organizations that cannot produce a well-documented breach record face adverse inferences in enforcement proceedings.
ICO Data Breach Reporting Form
The ICO’s breach reporting form is accessed through the ICO’s online portal at ico.org.uk and is structured to gather the information required under UK GDPR Article 33. The form walks reporters through a sequential intake process covering the nature of the breach, the data and individuals affected, the likely consequences, and the response measures taken.
The ICO’s form includes specific fields for: the type of personal data involved; the estimated number of individuals affected; the estimated number of records involved; the type of breach (confidentiality, integrity, or availability); and the cause of the breach. It also asks whether the breach is ongoing at the time of reporting, which affects the ICO’s prioritization of the case and the urgency with which it may seek additional information.
One practical consideration when using the ICO form is that it does not require the reporter to have precise figures for affected individuals or records; approximate numbers are explicitly acceptable at the initial filing stage. Organizations should resist the temptation to delay filing while counting exact records. Filing with reasonable estimates and supplementing later is both permitted and preferred by the ICO over a complete report submitted after the 72-hour window has closed.
PIPEDA Breach Report Form
The OPC provides a breach report form for PIPEDA notifications on its website at priv.gc.ca. The form is structured to capture the minimum information required under PIPEDA’s mandatory breach reporting regulations and can be submitted electronically to the OPC’s breach reporting address.
The form collects: the organization’s name, contact information, and privacy officer details; the date the breach occurred (if known) and the date it was discovered; a description of the breach including how it happened; the types of personal information involved; the number of individuals affected; the steps the organization has taken or plans to take to reduce the risk of harm; and whether affected individuals have been notified, and if not, when and how notification is planned.
Organizations should also complete the OPC’s accompanying breach of security safeguards record. This separate internal document must be maintained for 24 months for every breach, regardless of whether it meets the real risk of significant harm threshold. The OPC can request access to these records at any time, and failure to maintain them is independently enforceable under PIPEDA. The record and the breach report form together constitute the minimum documentation standard for PIPEDA compliance following any security incident involving personal information.
Mandatory Breach Reporting, Obligations You Can’t Ignore
Mandatory breach reporting is the legal requirement that organizations notify regulators and affected individuals after a qualifying data breach, without the discretion to decide whether disclosure is warranted based on internal business considerations. Across every major jurisdiction that has enacted privacy law in the past decade, the direction of travel has been toward mandatory reporting, broader scope, shorter timelines, and higher penalties for non-disclosure.

The shift from voluntary to mandatory reporting frameworks reflects a regulatory consensus that organizations left to decide for themselves whether to disclose breaches systematically underreport them. Mandatory reporting removes that discretion where it matters most: when personal data has been compromised, and individuals need to take protective action.
What Is Mandatory Data Breach Reporting?
Mandatory data breach reporting is a legal obligation, imposed by statute or regulation, that requires organizations to notify a designated authority, affected individuals, or both when a qualifying breach of personal data occurs, regardless of whether the organization believes disclosure is in its interest. The Word mandatory distinguishes these requirements from voluntary disclosure frameworks, which previously allowed organizations to self-assess whether a breach warranted public disclosure.
The practical meaning of ‘mandatory’ is that the decision to report is not a judgment call; it is a compliance determination. Once an organization concludes that a breach meets the applicable regulatory threshold, notification is required. The only discretion that remains is in timing, format, and content, all of which are themselves constrained by regulatory requirements. Organizations that treat mandatory breach reporting as optional, or that conduct a cost-benefit analysis of whether to disclose, expose themselves to enforcement action entirely separate from any penalty related to the breach itself.
Which Regulations Require Mandatory Reporting?
The list of regulations that impose mandatory breach reporting obligations has grown substantially over the past decade and now covers the majority of organizations that handle personal data in any significant volume. GDPR and UK GDPR mandate notification to supervisory authorities within 72 hours for breaches posing a risk to individuals’ rights and freedoms, with mandatory individual notification when the risk is high. HIPAA mandates notification to HHS OCR, affected individuals, and in some cases the media within 60 days of discovery of any reportable breach. PIPEDA mandates notification to the OPC and affected individuals when a breach creates a real risk of significant harm.
In the United States, all 50 states and several territories have enacted mandatory breach notification laws, making the US the jurisdiction with the broadest mandatory reporting coverage by sheer number of applicable statutes. The SEC’s cybersecurity disclosure rules require public companies to file Form 8-K for material cyber incidents within 4 business days. Australia’s NDB scheme mandates notification to the OAIC and affected individuals for eligible data breaches. Canada’s PIPEDA, Quebec’s Law 25, and several other provincial laws require mandatory reporting at both the federal and provincial levels.
The global pattern is consistent: wherever personal data is processed at scale, mandatory breach reporting has become the regulatory norm rather than the exception.
Near-Miss Data Breaches, Do They Need to Be Reported?
A near-miss data breach, an incident where a breach nearly occurred but was prevented before personal data was actually accessed or disclosed, does not trigger mandatory reporting obligations under most frameworks, because the legal definitions of a reportable breach require that unauthorized access or disclosure actually occurred, not merely that it was possible.
Under GDPR, a breach is defined as a security incident leading to the accidental or unlawful destruction, loss, alteration, unauthorized disclosure of, or access to personal data. An incident where data was at risk but access was blocked, a ransomware attack where encryption was prevented before it completed, for example, or a phishing attempt that was caught before credentials were used, does not meet this definition and is not reportable.
However, near-miss incidents carry their own documentation obligation under most frameworks. GDPR’s accountability principle requires controllers to document all security incidents, including those that do not meet the notification threshold, so that supervisory authorities can assess the adequacy of the controller’s security practices during an audit. PIPEDA’s breach record requirement extends to all breaches of security safeguards, whether or not they pose a real risk of significant harm, thereby capturing many near-miss scenarios. Organizations that rigorously document near-misses tend to identify systemic vulnerabilities before they result in a reportable breach.
Annual Breach Reporting Deadlines and Schedules
Some breach reporting frameworks include annual reporting obligations that operate on a calendar schedule rather than, or in addition to, the incident-triggered notification timelines. Understanding these scheduled deadlines is important because missing an annual filing can constitute a compliance violation even when the underlying incidents were individually managed in compliance with incident-specific requirements.
Under HIPAA, covered entities that experienced breaches affecting fewer than 500 individuals during a calendar year must submit their annual breach log to HHS OCR within 60 days after the end of that calendar year. This means all small breaches discovered between January 1 and December 31 must be submitted to the portal by March 1 of the following year. Covered entities should maintain a running breach log throughout the year rather than reconstructing it at year-end; HHS OCR has found that year-end reconstruction frequently results in underreporting when incidents from earlier in the year are not well documented.
The SEC’s annual Form 10-K filing includes mandatory disclosure of the company’s cybersecurity risk management program, strategy, and governance, including board oversight of cyber risk. This annual disclosure is separate from the incident-specific Form 8-K obligation and applies to all registrants regardless of whether they experienced a material incident during the year. Organizations that experienced incidents during the year must ensure their annual 10-K disclosures are consistent with any Form 8-K disclosures made during the same period; inconsistencies between incident reports and annual disclosures are a known area of SEC scrutiny.
Consequences of Failing to Report a Data Breach
The consequences of failing to report a data breach, whether through non-disclosure, late disclosure, or inadequate disclosure, extend across financial penalties, reputational damage, regulatory scrutiny, and civil liability, and they consistently exceed the consequences organizations hoped to avoid by not reporting.
Financial penalties are the most quantifiable consequence. Under GDPR, fines for notification failures can reach €10 million or 2 percent of global annual turnover. Under HIPAA, civil monetary penalties for breach notification failures are tiered by culpability: $100 per violation for unknowing violations, $1,000 for reasonable cause, $10,000 for willful neglect corrected, and $50,000 for willful neglect not corrected, with annual caps of $1.9 million per category. Under PIPEDA, failure to report a breach or maintain breach records is an offense under the statute carrying fines of up to CAD $100,000. State AG offices in the US have pursued multi-million-dollar settlements for breaches of breach notification requirements.
Beyond the immediate financial penalty, regulatory investigations triggered by late or inadequate reporting often expand in scope. A regulator that begins by investigating a notification failure frequently examines the underlying security practices that enabled the breach, the adequacy of the organization’s data protection program, and whether the breach was symptomatic of systemic compliance failures. Organizations that might have faced a limited inquiry for the underlying breach find themselves subject to a comprehensive compliance audit because the notification failure provided the regulatory foothold for a broader investigation.
Industry Data Breach Reports, Benchmarks and Statistics
Industry data breach reports are annual publications produced by research organizations, cybersecurity firms, and government agencies that aggregate breach data across thousands of incidents to identify trends, quantify costs, and benchmark organizational security performance. They are among the most cited sources in cybersecurity policy, regulatory guidance, legal proceedings, and boardroom risk discussions, and understanding what the major reports measure, how they differ, and what the most current findings show is essential context for any organization managing breach risk.

IBM / Ponemon Cost of a Data Breach Report (2024)
The IBM Cost of a Data Breach Report, produced annually in partnership with the Ponemon Institute, is the most widely referenced benchmark for the financial impact of data breaches on organizations globally. The 2024 edition, based on research conducted across 604 organizations in 17 industries and 16 countries, found that the global average cost of a data breach reached $4.88 million, a 10 percent increase over 2023 and the highest figure recorded in the report’s history.
Several findings from the 2024 report are directly relevant to breach reporting strategy. Organizations that involved law enforcement in ransomware incidents saved an average of $1 million compared to those that did not, contradicting the common assumption that engaging authorities increases costs. Organizations with high levels of AI and automation in their security programs experienced breach costs that were $2.2 million lower than those with low AI adoption. And organizations that identified a breach through their own security teams contained it 61 days faster, on average, than those notified by an external party. This finding underscores the economic value of proactive monitoring over reactive discovery.
The report also tracks mean time to identify and contain breaches: in 2024, the average breach went undetected for 194 days. It took an additional 64 days to contain, bringing the total lifecycle to 258 days. Organizations that contained a breach in under 200 days saved an average of $1.1 million compared to those that took longer, making detection speed the single most impactful operational variable in breach cost outcomes.
Verizon Data Breach Investigations Report (DBIR), Key Findings
The Verizon Data Breach Investigations Report is published annually and is the most comprehensive analysis of breach causation and attack methodology available to the public. Based on analysis of tens of thousands of security incidents and thousands of confirmed breaches submitted by law enforcement agencies, CERTs, and private contributors, the DBIR provides a statistically grounded picture of how breaches actually happen, rather than how organizations assume they happen.
The 2024 DBIR found that the human element was involved in 68 percent of breaches, consistent with prior years and underscoring that technical controls alone are insufficient without corresponding attention to social engineering, credential theft, and insider risk. Ransomware and extortion attacks accounted for 32 percent of all breaches, a figure the report notes is likely understated due to significant underreporting, particularly among mid-market organizations that lack the resources to conduct full forensic investigations and file complete regulatory reports.
The DBIR is particularly valuable for understanding which attack vectors are most prevalent in specific industries. Healthcare, financial services, and the public sector consistently rank among the most heavily targeted verticals, with credential theft as the leading attack vector across all sectors. Organizations using the DBIR to benchmark their security posture should focus on industry-specific breakdowns rather than global averages, as breach patterns vary considerably by sector.
Identity Theft Resource Center (ITRC) Annual Data Breach Report
The Identity Theft Resource Center’s annual data breach report is the primary public-facing source for tracking the volume of data breach notifications issued in the United States. Unlike the IBM/Ponemon report, which focuses on breach costs, and the DBIR, which focuses on breach causation, the ITRC report tracks notifications, how many breaches were disclosed, to how many victims, in which industries, and through which breach types.
The ITRC’s 2023 Annual Data Breach Report found that the number of data compromises in the United States reached 3,205, a 78 percent increase over the previous record set in 2021 and the highest figure the ITRC has recorded. The number of victims, however, declined significantly compared to prior years, a pattern the ITRC attributes to a shift in attacker behavior: criminals are increasingly targeting smaller, more specific datasets, employee records, credentials, customer subsets, rather than the massive consumer database breaches that characterized earlier years.
The ITRC report is particularly useful for compliance teams tracking notification volume trends, state-level breach patterns, and industry-specific breach frequency. It is also one of the few public sources that attempts to track the completeness of breach notifications, the proportion of breach notices that include all information required by applicable state law, and consistently finds that a significant percentage of notices omit required content.
Number of Data Breaches Reported in 2023 and 2024
The number of data breaches formally reported to regulatory authorities and published in breach notification databases has increased substantially in recent years, driven by both a genuine increase in attack frequency and an expansion of mandatory reporting requirements that capture incidents that would previously have gone undisclosed.
In the United States, the ITRC recorded 3,205 data compromises in 2023, affecting an estimated 353 million individuals, according to victim notices. In the UK, the ICO received approximately 3,000 breach reports in 2023, a figure that represents only breaches meeting the UK GDPR notification threshold and excludes the much larger volume of incidents that organizations determined were below the reporting threshold. The OAIC’s NDB scheme in Australia recorded 483 eligible data breach notifications in the first half of 2024 alone, with the health sector accounting for the largest share.
These figures almost certainly underrepresent the true volume of breaches. Regulatory surveys and academic research consistently find that a significant proportion of qualifying breaches go unreported, either because organizations incorrectly determine they are non-reportable, because they are undetected, or because organizations deliberately avoid disclosure. The DBIR’s finding that ransomware is involved in 32 percent of breaches but appears in a far smaller proportion of regulatory notifications reflects this underreporting gap, which is itself a focus of increasing enforcement attention from regulators in the EU, UK, and US.
FBI Internet Crime Report, Data Breach Victims and Losses
The FBI’s Internet Crime Complaint Center (IC3) publishes an annual Internet Crime Report that compiles cybercrime complaints submitted by the public and private sectors to the IC3 throughout the year. The report includes data on personal data breach victims and associated financial losses, providing a law enforcement perspective on breach impact that complements the regulatory and research-focused data in other annual reports.
The IC3’s 2023 Internet Crime Report recorded over 880,000 complaints, the highest volume in the IC3’s history, with total reported losses exceeding $12.5 billion. Personal data breaches accounted for a significant portion of complaints, with identity theft and credential compromise consistently ranking among the top crime types by victim volume. Business email compromise, which frequently involves the compromise of employee credentials and can trigger data breach notification obligations, remained the highest-loss crime category, generating over $2.9 billion in reported losses.
The IC3 report is particularly valuable for understanding the downstream consumer impact of breaches: what crimes are committed using the data after it is compromised. This downstream harm data is directly relevant to the harm-risk assessments organizations must conduct under HIPAA, GDPR, PIPEDA, and similar frameworks, because regulators expect those assessments to consider realistic harm scenarios, and the IC3 data provides empirical grounding for what those scenarios look like in practice.
What Annual Breach Reports Reveal About Reporting Failures
Taken together, the major annual breach reports reveal a consistent and troubling pattern: a substantial proportion of data breaches that should be reported under applicable regulations are not reported, are reported late, or are reported with incomplete information. This underreporting gap has become a focus of regulatory attention and enforcement in the EU, UK, and US.
The DBIR’s finding that breaches go undetected for an average of 194 days is one dimension of the problem; organizations cannot report breaches they have not detected. But a separate dimension, documented in the ITRC’s analysis of notification content and the ICO’s published enforcement decisions, is that organizations that do detect breaches frequently delay reporting while conducting internal investigations, misjudge whether breaches meet the reporting threshold, or file notifications that omit required content. The ICO has noted in its annual reports that a significant proportion of the breach reports it receives are filed after the 72-hour deadline, and that late-filing organizations rarely provide adequate justification for the delay.
The practical lesson from these reports for compliance teams is that breach-reporting failures are common, regulators are aware of this, and enforcement is shifting from breaches themselves to the adequacy of the reporting process. Organizations with mature incident response programs, clear escalation protocols, pre-mapped regulatory obligations, pre-built notification templates, and regular tabletop exercises consistently demonstrate better reporting outcomes than those that treat breach response as an improvised exercise.
How to Monitor for Breaches Before You Have to Report Them
The most effective breach reporting strategy begins before a breach occurs, with monitoring capabilities that detect compromised data, exposed credentials, and active threat activity early enough to intervene before a reportable incident crystallizes. Early detection does not eliminate the reporting obligation when a breach occurs. Still, it dramatically reduces the scale of what must be reported, the number of individuals affected, and the costs that follow.

Dark Web Monitoring as an Early Breach Detection Layer
Dark web monitoring provides visibility into the underground marketplaces, forums, and data dumps where compromised credentials, stolen records, and breached databases are bought, sold, and traded after an attack. When an organization’s data appears in these channels, it is almost always the result of a breach, and detecting that appearance on the dark web is frequently how organizations first learn of it, often before their own internal systems generate an alert.
The intelligence value of dark web monitoring is in the timing. Breached data typically appears on dark web markets within days to weeks of the underlying attack, and in many cases significantly before the organization has detected any anomaly in its own environment. The IBM 2024 report’s finding that breaches go undetected for an average of 194 days illustrates the detection gap that dark web monitoring is specifically positioned to close. An organization that learns its employee credentials are being sold on a dark web forum on day 7 after an attack has 187 days of advantage over one that discovers the breach through internal detection alone.
For compliance purposes, early detection through dark web monitoring also affects the regulatory timeline. Breach notification deadlines run from the date of awareness, and awareness established through proactive monitoring, rather than regulator or third-party notification, gives organizations control over the starting point of that clock and the ability to begin their internal assessment and response process before external pressure forces the issue.
How DeXpose Alerts You Before a Breach Becomes a Compliance Crisis
DeXpose monitors dark web markets, ransomware leak sites, criminal forums, malware logs, and stealer log repositories in real time, alerting organizations the moment their data, employee credentials, customer records, domain assets, or brand identifiers appear in compromised data sources. The platform is designed specifically to provide the earliest possible warning of a breach, giving security and compliance teams the time they need to assess, contain, and respond before a regulatory clock starts running under the worst possible conditions.
When DeXpose detects a match- a corporate email address in a stealer log, a domain appearing in a ransomware leak, or credentials associated with an organization’s systems being traded on a criminal marketplace- it generates an alert with the source, the data type, the date of appearance, and contextual threat intelligence about the likely origin and scope of the exposure. This is not raw data; it is actionable intelligence that a compliance team can use directly in a risk assessment and reportability determination.
For organizations operating under GDPR, HIPAA, PIPEDA, or any other mandatory reporting framework, the difference between discovering a breach through DeXpose on day 3 and discovering it through a regulator notification on day 60 is the difference between a managed compliance response and a crisis. Early detection is not just a security advantage; it is a compliance advantage.
[Start your free dark web report at dexpose.io/free-darkweb-report/]Free Dark Web Report, See If Your Data Is Already Exposed
DeXpose’s free dark web report gives organizations an immediate snapshot of their current exposure across dark web sources, including data breach repositories, criminal marketplaces, stealer logs, and leak sites. The report covers corporate email domains, employee credentials, customer data, and brand assets, and is generated instantly without requiring a sales conversation or a technical integration.
For many organizations, the free report is the first time they have seen a consolidated picture of what data associated with their domain is already circulating in compromised data channels. The results frequently reveal historical breach exposure that was never detected internally, credentials from breaches that occurred years ago, records appearing in aggregated leak databases, or domain mentions in threat actor communications. This historical exposure is itself a risk: credentials from old breaches remain active attack vectors as long as passwords have not been changed and multi-factor authentication has not been enforced.
The report takes less than two minutes to generate and requires only a domain or email address. For compliance teams assessing whether a current incident may have a dark web dimension, or for security teams conducting a baseline exposure assessment, it provides immediate, actionable intelligence, at no cost.
Frequently Asked Questions (FAQ’s)
How long do you have to report a data breach?
The deadline depends on which regulation applies: the GDPR and UK GDPR require notification to the supervisory authority within 72 hours of becoming aware; HIPAA allows 60 days from discovery; and the SEC requires a Form 8-K filing within 4 business days of a materiality determination. US state laws vary from 30 days to “without unreasonable delay,” which regulators typically interpret as 30 to 45 days in practice.
Do you have to report every data breach?
No, but the threshold for non-reporting is narrow and must be supported by documented evidence, not assumption. Under HIPAA, every impermissible PHI disclosure is presumed reportable unless a four-factor risk assessment affirmatively demonstrates low probability of compromise; under GDPR, notification is required whenever a breach poses a risk to individuals’ rights and freedoms, which covers most incidents involving identifiable personal data.
Who is responsible for initially reporting a breach?
The data controller, the organization that determines the purpose and means of processing personal data, bears primary responsibility for reporting to the relevant supervisory authority and notifying affected individuals. Under HIPAA, the covered entity holds this responsibility; under GDPR, it is the data controller; processors and business associates must notify the controller promptly, but the regulatory filing obligation rests with the controller.
What happens if you don’t report a data breach on time?
Late or non-reporting is treated as a standalone compliance violation separate from the underlying breach, subject to its own penalties. Fines can reach €10 million or 2 percent of global turnover under GDPR, up to $1.9 million per violation category under HIPAA, and millions in state AG settlements in the US, and regulators routinely expand the scope of their investigation when late reporting indicates broader compliance failures.
How do I report a data breach under GDPR?
File an initial notification with your lead supervisory authority through their designated online portal, for example, the ICO portal in the UK or your relevant national DPA’s portal in the EU, within 72 hours of becoming aware of the breach, with whatever information is available at that point. You can supplement the initial report with additional details as your investigation progresses; regulators prefer a timely incomplete report over a complete report filed after the deadline.
What is the proper way to report a PII breach?
Federal agencies and DOD organizations must report PII breaches to US-CERT within one hour of discovery, then conduct a harm assessment to determine whether individual notification is required within 10 days. Private sector organizations must identify every state law applicable to the affected individuals’ states of residence and notify both the relevant state attorneys general and affected individuals within the shortest applicable deadline, which varies from 30 days to “without unreasonable delay” depending on the state.
Who do you report a PHI breach to?
Covered entities report PHI breaches to HHS OCR through the breach reporting portal at ocrportal.hhs.gov, to affected individuals within 60 days of discovery, and to prominent media outlets in the relevant area if the breach affects 500 or more residents of a specific jurisdiction. Business associates do not report directly to HHS OCR; they notify the covered entity, which then carries the regulatory and individual notification obligations.
Can a data breach be reported anonymously?
No, major breach reporting frameworks explicitly require the notifying organization to identify itself, provide contact details for a designated privacy officer or DPO, and remain available for regulatory follow-up. GDPR’s Article 33, HIPAA’s portal submission process, and equivalent requirements under PIPEDA and the NDB scheme are all built on the principle of organizational accountability, which is structurally incompatible with anonymous reporting.
What is a notifiable data breach?
A notifiable data breach is a security incident involving personal data that meets the harm-risk threshold defined by the applicable regulation, creating a legal obligation to notify the relevant supervisory authority, affected individuals, or both. Under GDPR, it is a breach likely to result in a risk to rights and freedoms; under HIPAA, it is an impermissible PHI disclosure that cannot be shown to carry a low probability of compromise; under PIPEDA, it is a breach creating a real risk of significant harm to individuals.
How do near-miss breaches factor into reporting obligations?
Near-miss incidents, in which unauthorized access was prevented before personal data was accessed or disclosed, generally do not trigger mandatory notification obligations because most regulatory definitions require that unauthorized access or disclosure actually occurred. However, near-misses must still be documented under GDPR’s accountability principle and PIPEDA’s breach record requirements, and recurring near-misses within the same system or process are recognized indicators of systemic security weaknesses that regulators may scrutinize during audits.